Cystic pancreatic lesions Radiology Key

MR Imaging of Cystic Lesions of the Pancreas RadioGraphics
Computed tomography and magnetic resonance imaging are excellent modalities for both initial detection and characterization of cystic pancreatic lesions. An imaging classification system for these lesions has been proposed that is based on the morphologic features of the lesion.

MR Imaging of Cystic Lesions of the Pancreas RadioGraphics
Publicationdate 2021-08-01. This is the second version of the role of CT in staging pancreatic cancer. Pancreatic cancer is the fourth largest cause of cancer death in the United States and Europe with over 100,000 deaths per year in Europe alone. The overall 5-year survival ranges from 2-7 % and has hardly improved over the last two decades.
The Radiology Assistant Pancreas Cystic Lesions
Introduction Temporally, two phases of acute pancreatitis are identified in the Revised Atlanta Classification: Early - first week Only clinical parameters are important for treatment planning and are determined by the systemic inflammatory response syndrome - SIRS, which can lead to organ failure. Late - after the first week
Cystic pancreatic lesions Radiology Key
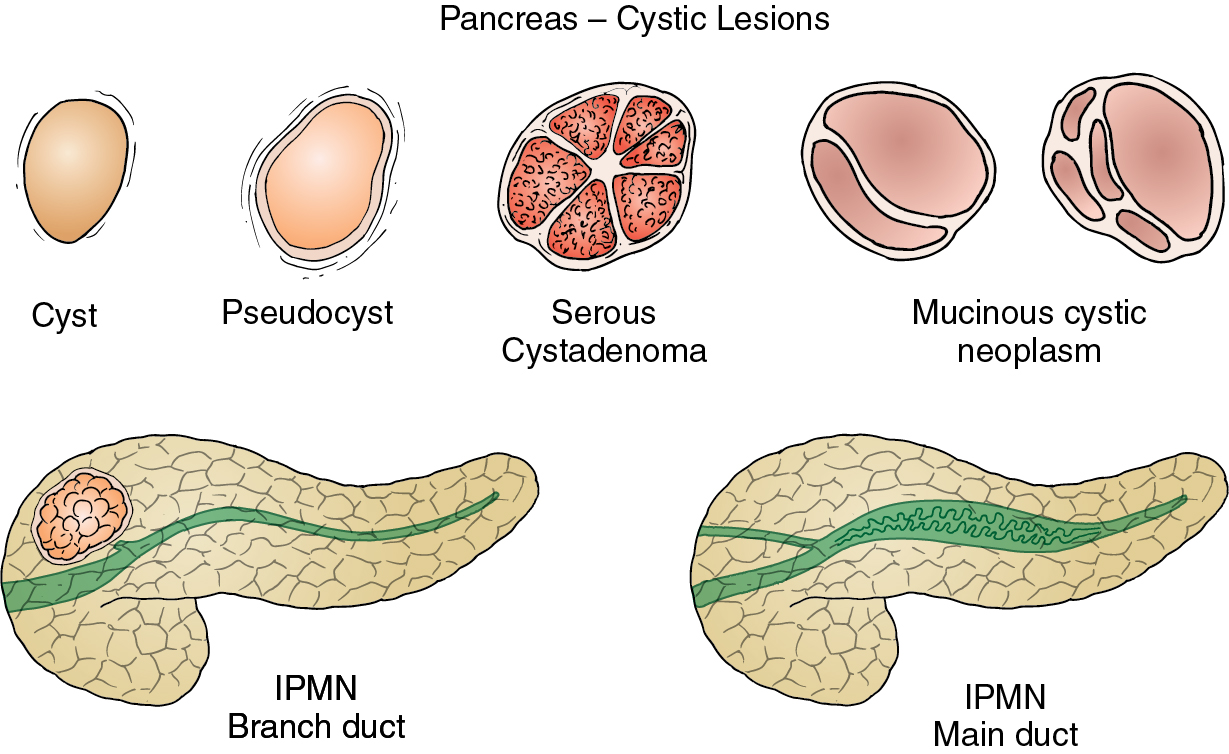
The most common cystic lesions of the pancreas seen on imaging are pseudocysts, serous cystadenoma, mucin-containing lesions (IPMN, mucinous cystadenoma, or cystadenocarci-noma), and solid papillary epithelial neoplasm. Other rare pancreatic cystic lesions include true epithelial cysts, cystic islet cell tumors, and adenocarcinoma with cystic.

The Radiology Assistant Pancreas Cystic Lesions
The purpose of this review is to outline the management guidelines for the care of patients with cystic pancreatic lesions. CONCLUSION. The guidelines are as follows: Annual imaging surveillance is generally sufficient for benign serous cystadenomas smaller than 4 cm and for asymptomatic lesions.
The Radiology Assistant Pancreas Cystic Lesions
glucagonoma cystic teratoma metastases to pancreas Retroperitoneal lesions (extrinsic to the pancreas) can mimic pancreatic cystic lesions, when close to the gland. Examples include: cystic lymphadenopathy (e.g. necrotic) duodenal diverticulum

MR Imaging of Cystic Lesions of the Pancreas RadioGraphics
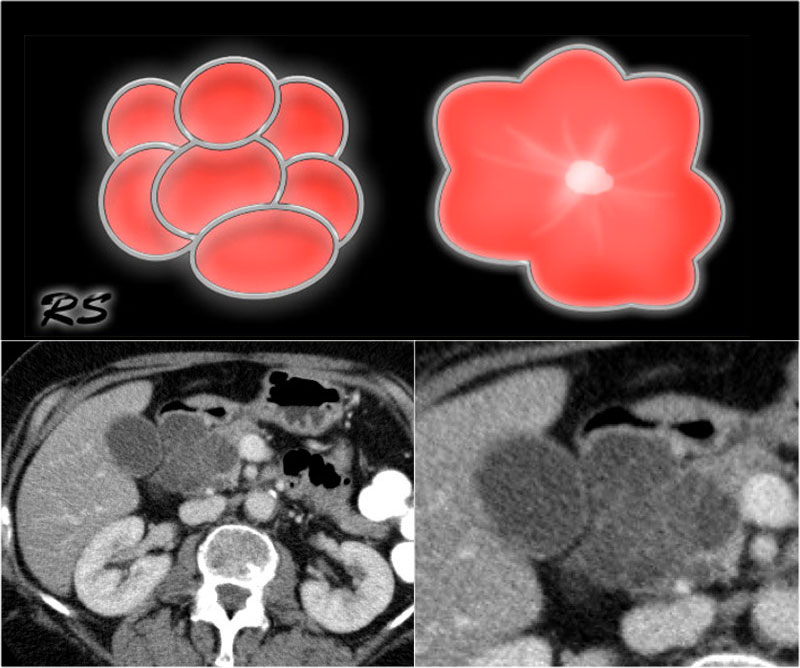
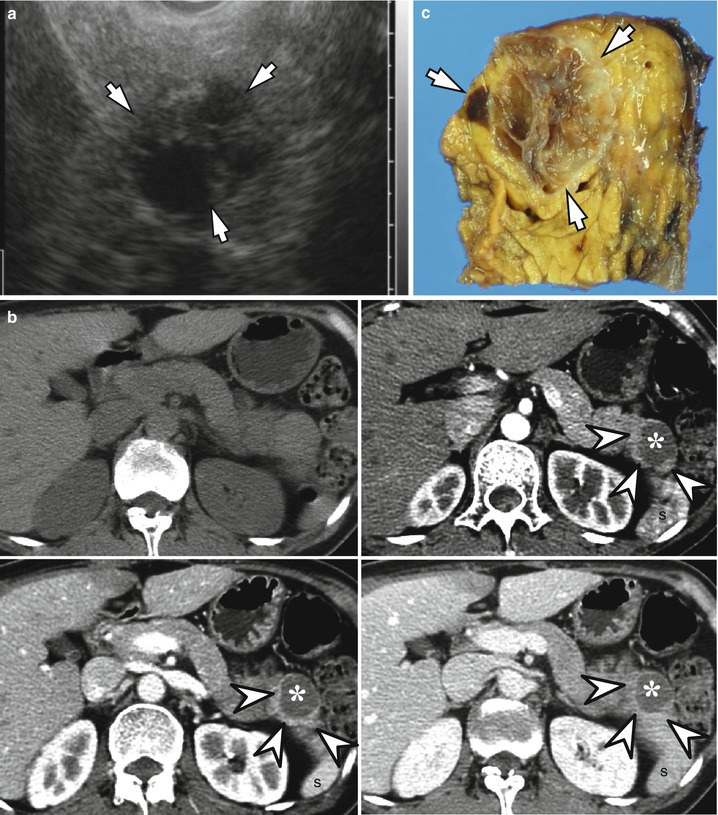
microcystic serous cystadenoma: usually head; 30% have a central scar cystic with a solid component macrocystic tumors can have a solid component as well pancreatic adenocarcinoma may undergo cystic degeneration (8%) 6 generally solid

Incidental Pancreatic Cysts on CrossSectional Imaging Radiology Key
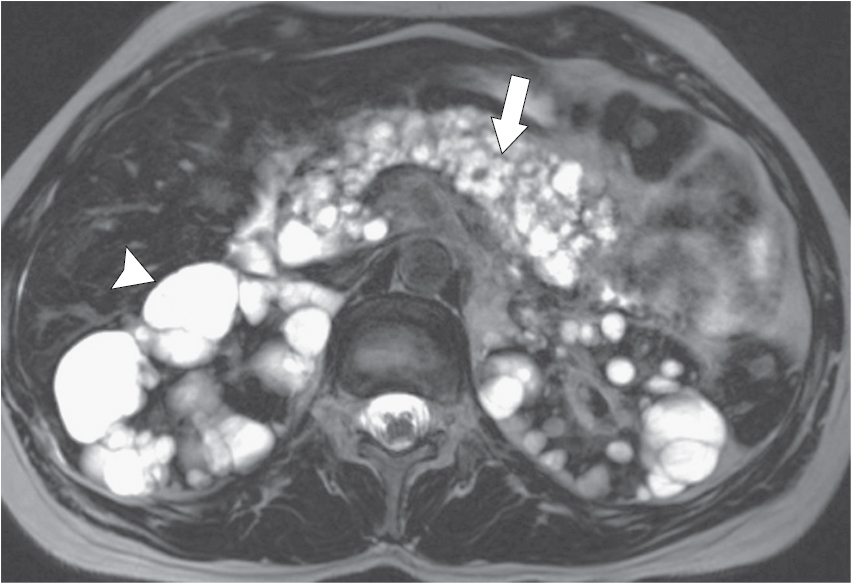
Pancreatic cystic lesions (PCLs) are present on up to 49% of abdominal magnetic resonance imaging (MRI) exams making these a common incidental finding, one that likely increases with age. 1 Definitions vary but a PCL is generally considered to be any closed sac-like structure with fluid or semi-fluid content within the pancreas on imaging, with or without communication with the main pancreatic.
Cystic pancreatic lesions Radiology Key
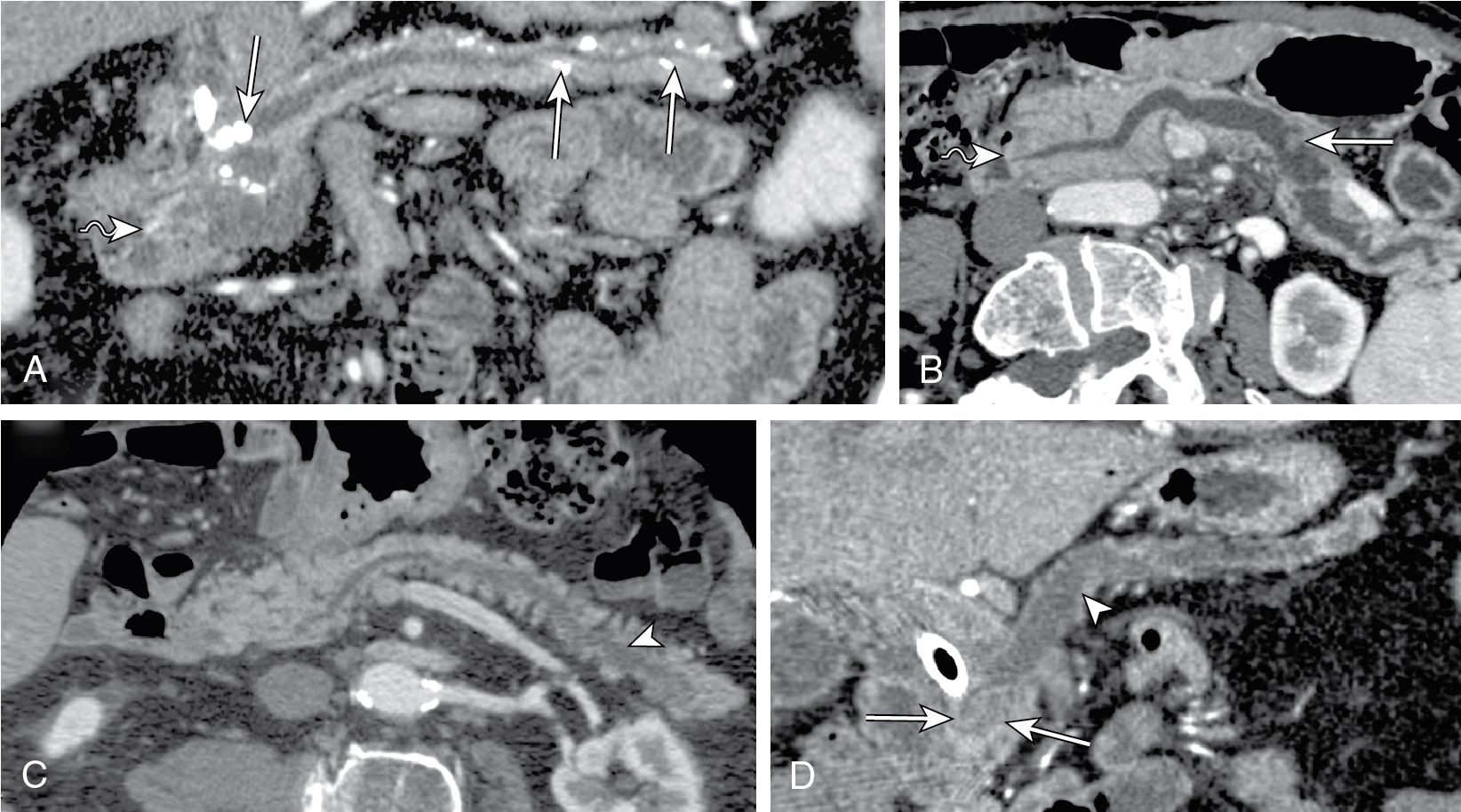
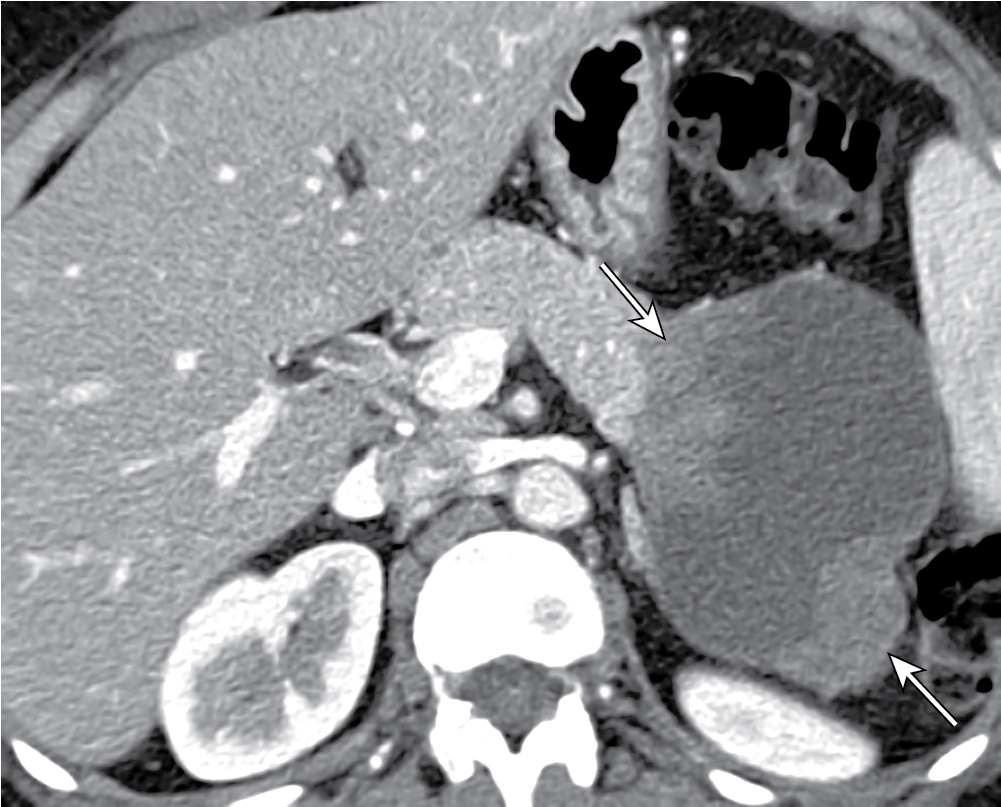
Pancreatic cystic lesions are relatively common imaging findings and may be secondary to both benign and malignant disease processes. Accurate characterization of the internal features of a cyst—including fluid, hemorrhage, septa, and enhancing soft-tissue components—is important to guide the differential diagnosis, and cross-sectional magnetic resonance (MR) imaging is the optimal.

Cystic Pancreatic Lesions A Simple Imagingbased Classification System for Guiding Management
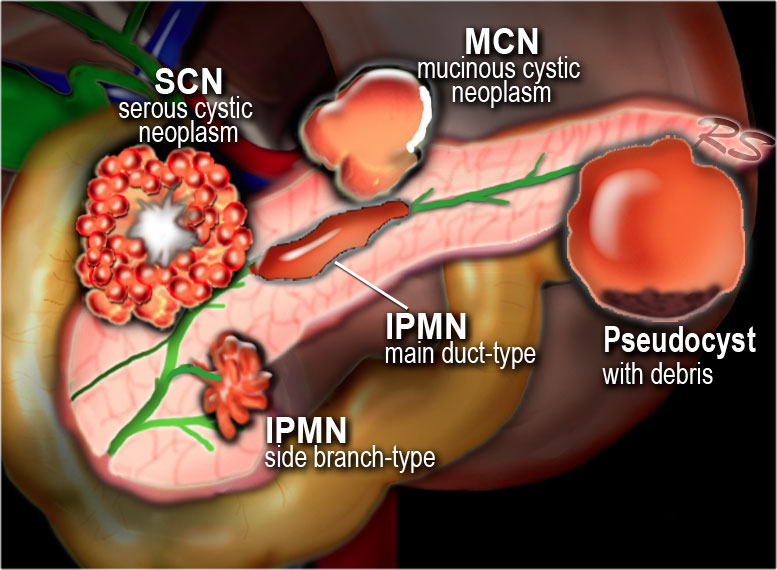
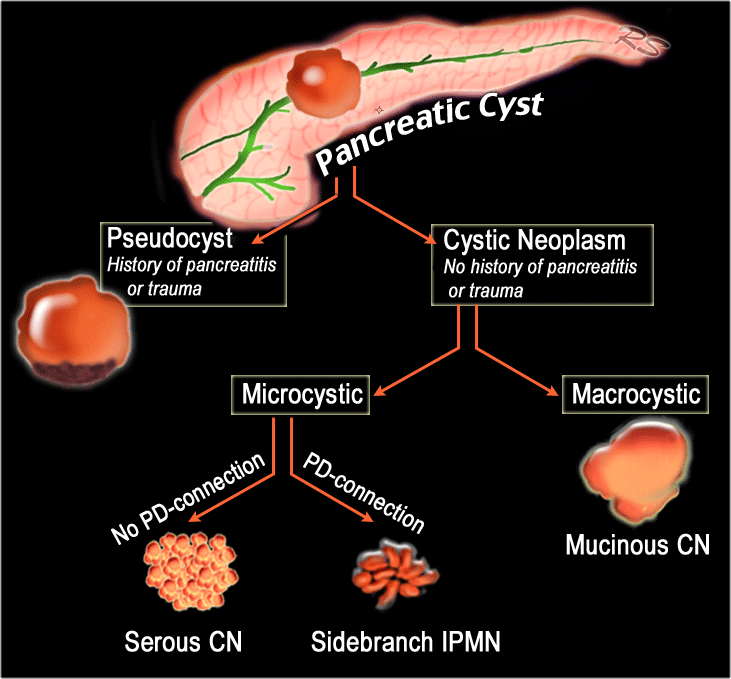
Introduction Classification Pancreatic cysts can be categorized into the following groups: Pseudocysts Common cystic neoplasms: IPMN - intraductal papillary mucinous neoplasm SCN - Serous cystic neoplasm MCN - Mucinous cystic neoplasm Uncommon cystic neoplasms: SPEN (solid pseudopapillary epithelial neoplasm) Tumors with cystic degeneration:
The Radiology Assistant Pancreas Cystic Lesions
Cystic pancreatic lesions (CPLs) are frequently casual findings in radiological examinations performed for other reasons in patients with unrelated symptoms. As they require different management according to their histological nature, differential diagnosis is essential. Radiologist plays a key role in the diagnosis and management of these lesions as imaging is able to correctly characterize.

The Radiology Assistant Pancreatic cystic Lesions
Pancreatic cystic lesions are frequently identified on cross-sectional imaging. As many of these are presumed branch-duct intraductal papillary mucinous neoplasms, these lesions generate much anxiety for the patients and clinicians, often necessitating long-term follow-up imaging and even unnecessary surgical resections.
Cystic pancreatic lesions Radiology Key
CME Tools Share Abstract The widespread use of high-spatial-resolution cross-sectional imaging has led to an increase in detection of incidental pancreatic cystic lesions. These lesions are a diverse group, ranging from indolent and premalignant lesions to invasive cancers.
Cystic pancreatic lesions Radiology Key
The purpose of this review is to outline the management guidelines for the care of patients with cystic pancreatic lesions. CONCLUSION. The guidelines are as follows: Annual imaging surveillance is generally sufficient for benign serous cystadenomas smaller than 4 cm and for asymptomatic lesions.

The Radiology Assistant Pancreatic cystic Lesions
Pancreatic cystic neoplasms (PCN) comprise of a diverse array of pancreatic cysts, including intraductal papillary mucinous neoplasms (IPMN), mucinous cystic neoplasms (MCN), serous cystic neoplasms (SCN), cystic neuroendocrine tumors (cNET), and many others. Increasing use of cross-sectional imaging has resulted in greater numbers of PCNs discovered incidentally. The overall risk of.
Cystic Tumors of the Pancreas Radiology Key
Abstract. Although the probability of pancreatic cystic neoplasms (PCNs) being detected is raising year by year, their differential diagnosis and individualized treatment are still a challenge in clinical work. PCNs are tumors containing cystic components with different biological behaviors, and their clinical manifestations, epidemiology.
